VAGINOPLASTY – Surgical Tightening
Reconstructive Vaginoplasty
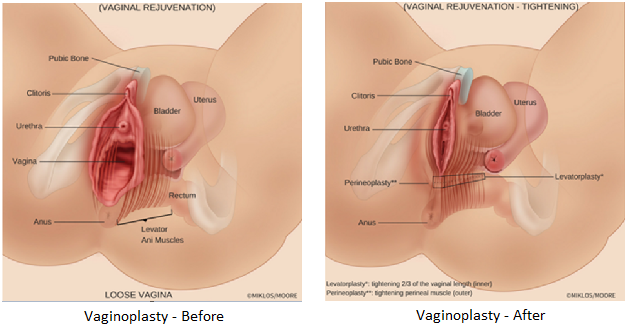
(Vaginal Rejuvenation)
Vaginoplasty
Cosmetic vaginoplasty also known as vaginal rejuvenation or vaginal tightening is most often performed due to a loose vagina, less friction or a lack of friction during intercourse. Lack of friction during intercourse is most commonly a result of vaginal childbirth, pregnancy, spinal and sacral nerve damage, excessive weight (ie high body/mass index), heavy lifting and chronic increases in abdominal pressure (straining for constipation, chronic coughing, lifting heavy weight all of which damages pelvic nerves and ultimately puts excessive pressure on the pelvic floor fascia (support tissue) and muscles.
The muscles of the pelvic floor are known as the levator ani muscles these are the same muscles that patients use during Kegel exercises. These muscles are the point of lateral attachment of the ceiling of the vagina and floor of the vagina. When nerves of the tailbone i.e. sacrum are damaged, this reduces the electrical impulse into the levator muscles and over time the fascia of the ceiling of the vagina and the floor of the vagina rip from the muscles resulting in further relaxation and vaginal prolapse. Vaginal prolapse can manifest as a cystocele (bladder drop), rectocele (rectum bulge), enterocele (intestinal bulge) and vaginal vault prolapse (the deepest portion of the vagina falls). It is impossible to fix the damaged nerves of the pelvic floor so options in therapy include strengthening the muscles by:
|
The options above only enhance or workout the muscles of the pelvic floor and do not treat the nerves nor the fascia. Since most patients with severe pelvic muscle and fascia damage can’t fix their problem with the above minimally invasive techniques the patients often turn to surgery which usually requires the patient have her prolapse fixed concurrently with the tightening of her vagina.
However, simply fixing the vaginal prolapse (i.e. cystocele, rectocele and vaginal vault prolapse) will not tighten the vagina!! All too often uninformed plastic surgeons, gynecologists, urologists and urogynecologist make this very mistake and the patient undergoes a surgical procedure with little benefit. Vaginal tightening is an art and requires training and experience to achieve the best outcomes.
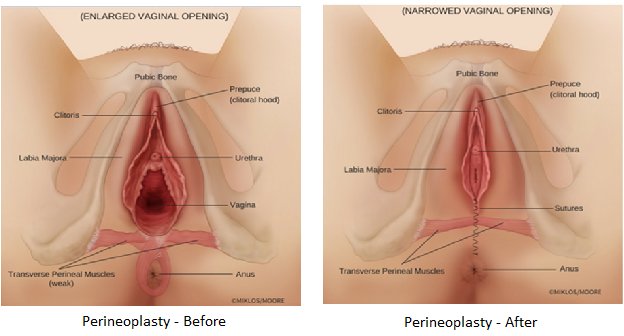
Many surgeons will attempt to tighten the vagina by only tightening the vaginal opening. This technique is known as a perineoplasty and by itself is a useless surgery if the patient wants to feel more friction during intercourse. It is functional if the patient wants her vagina to appear more less gaping or enlarged, but it is a fruitless operation for vaginal rejuvenation if performed by itself.
The key to a successful vaginal tightening procedure is choosing a surgeon with experience, expertise and one who has proven results. The surgeon should know his/her personal results and be able to covey the success rate to their patient. A surgeon cannot just say well the scientific paper states the success rate is 90% and suggest these are his/her success rates……that is simply ridiculous and would be like saying well LeBron James scores 30 points per game then you can too.
To achieve surgical success the surgeon needs to tighten more than just the opening of the vagina, he/she should tighten on average approximately 60-70% of the length of the vagina working from the inside towards and including the vaginal opening. The opening is repaired by doing a perineoplasty but a perineoplasty alone will not tighten the whole vagina and will not satisfy the average woman’s expectations of the surgery. The internal aspect of tightening includes the pulling of the levator ani muscles towards the midline and the perineoplasty requires reapproximation of the transverse perineal muscles. Ask you potential surgeon his/her success rate and then ask them: 1) how do you define success and 2) can you prove your results and finally 3) if it does not work do you provide any guarantee?