Tension-free Vaginal Tape Slings
(TVT – TOT – Single Incision Slings)
Sling operations for the treatment of stress urinary incontinence have been around for more than 100 years. Slings can be performed by using several materials including a patient’s own tissue (abdominal or leg fascia), cadaveric tissue, cow and pig skin as well as synthetic mesh.
Types of TVT Slings
In 1998, the first industry made synthetic mesh sling introduced into the USA was Johnson & Johnson’s Gynecare TVT sling. This device was produced and tested in Sweden between 1994-1998 and finally introduced into the USA at that time.
The TVT sling was the first sling with material quality assurance as well as surgical technique reproducibility. The TVT with a step-by-step guideline defined a reproducible technique previously not offered with traditional type slings. Though the reproducible technique was not perfect it was a cutting-edge new technology when compared to other anti-incontinence surgical procedures, techniques and devices. Surgeons fell in love with the technique/device as it was considered relatively safe, fast, effective and minimally invasive as the surgery was performed through very small ie miniature incisions in the vagina and on the lower abdomen.
Essentially the surgery was performed through one vaginal incision of 1 inch and two small pubic incisions of 1/3 and inch.
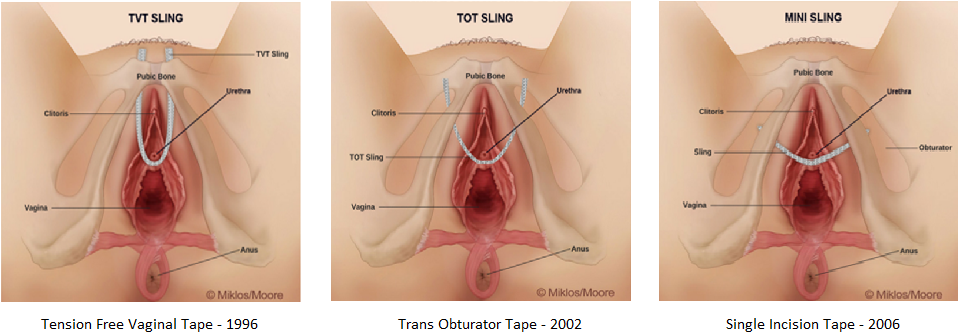
In 2002, the TOT sling also known as the transvaginal tape – obturator approach was introduced into the U.S.A. This sling had the same vaginal incision as the original TVT sling but it did not exit behind the pubic bone but instead the sling arms exited through the groin on each side of the vagina. This was initially thought to be a brilliant breakthrough because now the surgeons could avoid or decrease the chance of injury to the bladder or intestines. It was also felt that this pathway for the mesh sling would decrease bleeding. Overall these statements proved to be true, but what nobody realized with the potential for longer term and more devastating complications such as vaginal pain, groin pain, leg pain and painful intercourse. The scar tissue in the muscle and fascial layer of the groin which incorporated the mesh sling sometimes proves to be devastating and debilitating to some TOT recipients.
In 2006, the single incision sling or mini sling was developed and this was like the TOT slings however the sling did not have exit wounds in the groin. Instead the sling was inserted through the single midline incision under the skin beneath the urethra and directed to the pelvic sidewall.
Cure Rates
The TVT sling is the most studies anti leakage operation ever developed and has been studied over a period of more than 20+ years. The overall cure rates on average have often been described as:
90% 1 year after surgery
85% 5 years after surgery
80% 10 years after surgery
The TOT sling has had similar results however as stated above much more devastating and debilitating complications such as groin and leg pain. There are several papers suggesting that some single incision slings i.e. mini slings have similar cure rates at the TVT and TOT sling 5 years after surgery.
Complications
Initially the medical industry and surgeons felt there were few complications associated with synthetic mesh slings, however, over time patients have educated some surgeons, attorneys and the world that delayed, severe, chronic and life changing complications can occur. Complications associated with synthetic TVT sling surgery include: intraoperative, immediate post-operative and delayed post-operative.
Intraoperative complications include:
Bladder injury, urethral injury, bleeding ie hemorrhage, blood transfusions.
Immediate post-operative complications include:
Urgency, frequency, surgical failure, mesh exposure, urinary tract infections, vaginal pain, mesh and wound infection, and abscess formation.
Delayed post-operative complication include:
Vaginal pain, painful intercourse, vaginal mesh extrusion aka exposure, urethral erosion, bladder erosion, recurrent urinary tract infections, lower abdominal pain (TVT retropubic), groin pain (TOT), leg pain (TOT), and bowel erosion (TVT sling).
Complications are best addressed immediately especially when the complication is pain. Surgeons need to be aware of these potential complications so they can make the diagnosis and start initiating treatment. Failure to identify complications (especially pain) will delay therapy which can result in a more chronic, exaggerated, potentially debilitating chronic pain which may not be treatable or controllable in the future.